Laser Surgery and Anaesthesia
Dept of Anaesthetics, Royal Prince Alfred Hospital, Sydney,
Australia

Some of the section dealing with the physics of lasers was
written with the help of an article by David Tilbrook, published in
the July 1980 issue of Electronics Today International (ETI). That
magazine regrettably went out of print some years ago. David's
fascinating article was one of the things that sparked my interested
in electronics and I am grateful to him.
Part I. LASER PHYSICS
QUANTUM PHYSICS.
The universe contains two fundamental quantity types:
- Continuous e.g. velocity
- Quantised e.g. standing waves and harmonics
Many quantities in molecular, atomic and sub-atomic physics are
quantised. 'Classical Physics' assumed these were continuous and only
after the advent of Quantum Physics (c1900) were working models of
atomic structure and electromagnetic radiation possible.
QUANTUM PHYSICS AND LIGHT. 1.
Most light sources are heated solids or gases (e.g. electrically
heated tungsten filaments) emitting a spectrum of wavelengths, the
relative intensities of which are dependent on the temperature.
Classical physicists found there were too many variables to analyse
so to simplify things somebody invented the 'cavity radiator', simply
a hollow solid with a hole in the side. When heated to a particular
temperature the light from the hole is brighter than that from the
outside. It is also largely independent of the material used to make
the radiator and varies more simply with the temperature.
Nevertheless, classical physicists using the wave theory of light
still could not explain the relative intensities of the various
wavelengths of this cavity or 'black body' radiation.
In 1900 Max Planck realised that the atoms in the cavity were
behaving as electromagnetic oscillators which could emit light into
and absorb light from the cavity but only at characteristic
frequencies. He concluded that the atoms could not have a continuum
of different energies but only energies given by the equation:
E = nhv
where
- E = energy
- n = an integral number
- h = Planck's constant
- v = frequency (normally represented by greek letter
upsilon)
Also the atoms could not radiate continuously but only in 'quanta'
and only when the atom jumped from a high energy state to a lower
one. Planck, however, still thought of light as a wave.
QUANTUM PHYSICS AND LIGHT. 2.
If light is shone on a clean metal surface some electrons are
liberated from the metal - the photo-electric effect. If the metal is
put in a vacuum tube with an external circuit a measurable current
will flow. By then connecting this to a power supply the voltage
which just stops the photo-electric current can be measured and used
to calculate the energy of the photo-electrons. Several things become
apparent:
- Photo-electron emission begins as soon as the light comes
on.
- Current flow is proportional to light intensity.
- Photo-electron energy is proportional to light frequency -
(NOT intensity)
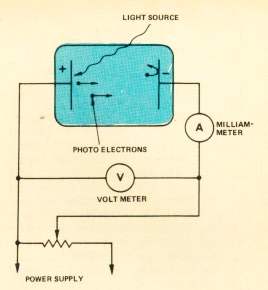
Fig.1. The Photo-electric Experiment
Classical physicists tried unsuccessfully to explain these
phenomena using wave theory.
In 1905 Albert Einstein applied Planck's theories to the problem
and was able to explain the observations. He postulated that light
was not continuous waves but quanta he called photons, each with
energy 'E' given by Planck's equation. Any single photon can interact
with a single electron so the energy imparted to this electron will
depend only on the energy of the photon and therefore its frequency.
Increasing the intensity of the light will increase the number of
photo-electrons released and hence the current. Emission will start
instantaneously since all the energy required for a photo-electron
release is contained in a single photon.
SPONTANEOUS AND STIMULATED EMISSION.
When a photon interacts with a bound electron it may not have
enough energy to overcome the binding forces. In this case the photon
is absorbed by the electron but the electron is not liberated from
the atom. Instead, it jumps to a higher energy level, forcing the
atom from its 'ground state' with energy 'E1' to a higher
energy level, say 'E2'. If the photons absorbed have
energy E = hv then the increase in electron energy will also be hv
i.e. E2 - E1 = hv.
After about 10-8 seconds the electron will drop back to
the ground state, re-emitting a photon, again with energy hv.
The excited atom has no preferred direction in space and so the
photon can be radiated in any direction while the atom recoils in the
opposite direction. This process is called spontaneous emission. If a
group of atoms are excited in this way they will radiate photons in
all directions randomly as the atoms return to their ground
states.
If however a photon with energy hv interacts with another electron
at energy level E2 the electron is forced down to its
ground state with the emission of a second photon. This is called
stimulated emission and is the basis for laser activity.
The most important point about stimulated emission is that both
photons leave the atom with the same phase, direction and wavelength
as the incoming photon. If they did otherwise they would interfere
and cancel thus violating the law of energy conservation. The two
photons are said to be coherent. If a group of atoms are excited in
this way the initial beam of photons will be augmented by the
additional photons and so is 'amplified'.
POPULATION INVERSION
If a material is in thermal equilibrium at a temperature T, the
distribution of atoms in a lower energy state to those in higher
states is normally heavily accented towards the lower state. If
N1 is the density of atoms in the lower state and
N2 the density of more excited atoms, then the ratio of
N2 to N1 is given by:
N2/N1 = e(kT/hv)
where
- T = temperature in Kelvin
- k = Boltzmann's constant
If the material is at 103K then
N2/N1 = 10-5 so only one atom in
105 is in the excited state!
The condition in which the number of excited atoms exceeds those
in the ground state is a non-equilibrium condition called population
inversion. This condition is necessary to maintain laser activity. If
the vast majority of atoms are in the ground state then only
absorption and spontaneous emission can occur. If a population
inversion can be maintained then stimulated emission will occur
leading to photon multiplication. The process used to maintain
population inversion is called pumping.
THE ACTUAL PHYSICS OF A LASER.
So how do you turn all this quantum physics into a laser? This is
probably best illustrated by example. Let's look at the helium-neon
laser which has a tube containing about 90% He and 10% Ne at a
pressure of one to three Torr, through which high voltage dc can be
passed.
Helium has energy levels at 20.61 and 19.82 electron volts (eV)
which are metastable. Once at a metastable energy level an atom
cannot move to a lower state by emission of a photon. It can only be
de-excited by some other process e.g. transfer of energy to another
atom. So, once an atom is excited to a metastable level it will stay
there for a long time, about 10-3 seconds, hence large
metastable populations can exist.
Two of neon's energy levels, 20.66 and 19.78eV, closely coincide
with the metastable levels of helium. Large amounts of metastable He
are produced by the electric discharge. Energy transfer will take
place between metastable He and ground state Ne producing large
populations of excited Ne atoms at 20.66 and 19.78eV. The population
of excited Ne atoms produced in this way vastly exceeds that
achievable by direct excitation by the electric discharge. Below
these two highly populated energy levels are two lower Ne energy
levels (20.3 and 18.7eV) that are only populated by direct excitation
and therefore have much lower populations. We have a population
inversion!
There are three possible transitions:
- 20.66 to 20.3eV producing 3391nm light (far infrared)
- 19.78 to 18.7eV producing 1152nm light (infrared)
- 20.66 to 18.7eV producing 633nm light (visible red light)
As Ne and He atoms jump between energy levels photons are emitted
randomly in all directions. Since there are many Ne atoms at the
20.66 and 19.78eV energy levels, any photon with one of the above
three wavelengths has a high probability of causing stimulated
emission of a second identical photon. Those photons travelling
parallel to the axis of the tube are reflected back and forth by
mirrors at each end of the tube giving rise to more and more
identical photons by stimulated emission. A limit is finally reached
when the rate of production of Ne atoms at the higher energy levels
equals the rate of stimulated emission.
One of the end mirrors is made a few percent transparent and a
portion of the coherent radiation can escape from the tube to become
the laser output. Although laser stands for light amplification by
stimulated emission of radiation the HeNe laser is not really an
amplifier but an oscillator generating coherent electromagnetic
radiation at three distinct frequencies.
Part II. LASER HARDWARE
WHAT SORTS OF LASER ARE THERE?
Solid State Lasers. In laser physics 'solid state' does not
refer to semiconductors but to a breed of laser having a medium that
is formed by 'doping' a crystalline or glass material with an
impurity which produces the laser action when pumped. The most common
of these is the ruby laser which consists of a central, cylindrical
synthetic ruby crystal made from aluminium oxide as a base material
doped with chromium as the impurity. The crystal is mounted with
mirrors at each end (the front one slightly transparent) and is
surrounded by a xenon flash tube which is the 'pump'. Optical pumping
is a requirement of all solid state lasers. The Nd-YAG laser falls
into this group as well. Its crystal is a garnet made from
yttrium-aluminium oxide doped with neodymium.
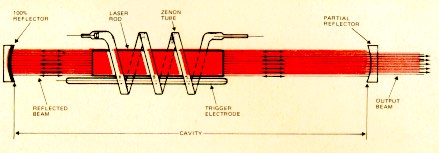
Fig.2. A Ruby Laser
Semiconductor Lasers. These are relatives of the LED, the
most common being the gallium arsenide laser consisting of a
semiconductor diode junction formed by GaAs doped with two different
impurities to form the p and n materials. When forward bias is
applied a large number of electrons and 'holes' move toward the
junction and recombine to generate the laser light. Power output is
low generally and efficiency is high. The output is easily modulated
making these very useful for optical communication.
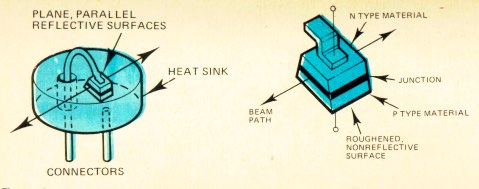
Fig.3. The Semiconductor Laser
Liquid Lasers. Most liquid lasers use an organic dye as the
laser medium and are optically pumped, sometimes by other lasers.
Their big advantage is that they are 'tunable'. This is achieved by
changing the dye for course tuning or by rotating a diffraction
grating for fine tuning of up to 50nm. Our most familiar liquid laser
is the Candela. Its 585nm light passes through dermal structures and
is strongly absorbed by HbO2 resulting in
thermocoagulation of the ectatic vessels in vascular skin lesions
(Selective Photothermolysis).
Gas Lasers. The HeNe laser is the most common in this group
and its workings have already been described in detail. Commonly used
medically are the CO2 and Argon lasers.
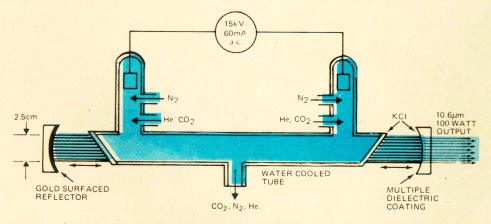
Fig.4. A CO2 Laser
OTHER BITS AND PIECES.
Frequency Doublers. These can be used to convert laser
light to a different, shorter wavelength. A beam of light passed
through a crystal of potassium-titanyl-phosphate (KTP) will emerge
with a mixture of the original wavelength and a wavelength one-half
the original (twice the frequency). In medical lasers, KTP is most
often used with Nd-YAG.
Light Guides direct the laser beam to the surgical site.
Fibreoptic bundles can be used for visible and near-infrared
wavelengths while wavelengths out of this range require either an
articulated arm containing front-surface mirrors at each joint or,
rarely, more exotic type fibreoptics. The light may then be focused
to the site by an operating microscope aimed using a lower power
(usually HeNe) beam, or it may be used to heat a contact probe
(usually sapphire tipped).
Part III. CLINICAL APPLICATIONS
ADVANTAGES OF LASER SURGERY.
Lasers have some unique advantages in surgery. They allow precise
microsurgery, even in difficult locations, by using fibreoptic
delivery for example. The types of surgery amenable to lasers
therefore includes all surface lesions and those accessible by
laparoscopy or endoscopy e.g. thoracic surgery, ophthalmology,
gynaecology, plastics, ENT, urology and neurosurgery.
The ability to focus the beam on a tiny area concentrates the
intensity enormously, producing heat at a rate of many thousands of
degrees in some cases, allowing precise, rapid vaporisation of
tissue.
Laser surgery is relatively dry, providing near instantaneous
sealing of small vessels and lymphatics. There is also minimal damage
to adjacent tissues resulting in less oedema, scarring and post
operative pain.
LASER INTERACTION WITH TISSUE.
Living tissue is basically an aqueous solution of light absorbing
molecules. When an atom interacts with a photon whose energy does not
exactly match a possible electron transition the atom is made to
vibrate and produce heat. The wavelength of the light determines its
degree of absorption. Other factors include the power density and
duration of the laser burst and the scatter, thermal conductivity and
local circulation of the tissue.
Long infrared wavelengths like that from the CO2 laser
(10,600nm) are completely absorbed by water in the first few layers
of cells leading to explosive vaporisation of the tissue surface and
little damage to underlying tissue. Excimer lasers in the ultraviolet
range are even more strongly absorbed by water and have an even more
superficial effect.
Near infrared from a Nd-YAG (1064nm) is much less absorbed by
water and the beam is transmitted and scattered through hundreds of
times more tissue than the CO2. This produces less
vaporisation and more thermal coagulation to a much deeper level
(i.e. a few mm).
Red light from a ruby laser (694nm) is poorly absorbed except by
cells containing dark pigment. The green (488nm) and blue (514nm)
light from an argon laser and similarly from the krypton laser (476,
521, and 568nm) is transmitted by water and intensely absorbed by
haemoglobin, thus penetrating skin and ocular structures to coagulate
vascular or pigmented lesions.
Infrared and visible lasers have exclusively thermal effects on
tissue but the ultraviolet photons from the excimer are energetic
enough to disrupt chemical bonds and cause ionisation potentially
leading to mutagenesis.
HAZARDS OF LASER SURGERY. 1. Non Airway Surgery.
Atmospheric Contamination. Tissue vaporisation by laser or
electrosurgery produces smoke plumes and fine particulates with mean
size 0.3mm. These can deposit in alveoli potentially causing
interstitial pneumonia, bronchiolitis and reduced mucociliary
clearance. It may also be mutagenic, laser smoke supposedly having
half the mutagenic potential of that produced during electrocautery.
Inhaling the smoke from a gram of tissue has been equated with 3-6
cigarettes. The smoke may also carry viral DNA or bacterial spores
but the infectivity of this is yet to be proven. Prevention is with
smoke evacuators and high efficiency masks (normal masks are
useless).
Venous Gas Embolism. This is a consideration with
laparoscopic laser surgery and also with laser probes that use
coaxial gas cooling systems. Saline coolant has been recommended over
gas but then there is the potential for TURP-like syndromes. Embolism
has also been reported during laser resection of tracheal
tumours.
Organ or Vessel Perforation. Vessels greater than 5mm
diameter will not be coagulated by laser. Pneumothorax has occurred
with laryngeal procedures. Burn depth is difficult to assess with
Nd-YAG lasers and perforation can occur days after the surgery when
oedema and necrosis peak.
Inappropriate Heat Transfer. Laser energy can potentially
strike anything in the theatre causing fires and damage to patients,
staff and equipment. Lasers should not be fired in any direction
except at the lesion. The light may be reflected from any polished
surfaces so dull or matt instruments should be used. If the light is
not in the visible range then another coloured one must accompany the
beam. Cover patients eyes with moistened pads or metal guards.
Theatre doors and windows must be covered and warning signs posted.
Moisten drapes to prevent ignition and have a bucket of water in the
theatre. Staff should wear goggles of appropriate colour with side
guards (clear plastic or glass for C02, green for Nd-YAG,
orange for argon).
HAZARDS OF LASER SURGERY. 2. Airway Surgery.
All the above hazards apply with the additional problems of shared
airways, potentially obstructing lesions, poor respiratory reserve in
many cases, and the potential for airway fires. All the usual
anaesthetic considerations for ENT surgery apply and will not be
discussed here.
The high energy of laser beams can perforate or ignite
endotracheal tubes, and anaesthetic gases vigorously support
combustion potentially causing 'blowtorch' fires. The incidence of
this is between 0.5 and 1.5% in the USA.
Relative Flammability. The data about the relative
flammability of various types of ETT is conflicting. Many other
factors are important such as the amount of blood and mucous present
and the type of laser. The composition of the anaesthetic gases is
also important. PVC tubes produce more toxic substances than red
rubber and while silicone is harder to ignite it produces silica ash
when it burns which may be blown far down into the lungs.
Gas Composition. The minimum FiO2 should be used
to maintain oxygenation and N2O must be avoided. Other
diluents should be used such as air or He, the lower density of which
may be of advantage in airway obstruction, and its higher thermal
conductivity may help prevent fires. The volatile agents are not
flammable in clinical concentrations but can't be used in venturi
systems.
Protective Taping. Muslin saturated with water and wrapped
around the ETT has been used but it catches fire when dry so epidural
catheters have been taped on as well to keep the muslin wet. More
popular these days are foil tapes of aluminium, copper or metallised
plastic. Copper appears to be best and the plastic ones are generally
useless. A single length of 1/4 inch wide adhesive backed tape (tapes
specially made for this purpose are available) should be wrapped
spirally and overlapping from the cuff to the pilot tube entry point.
This method of tube protection is cheap and generally effective but
risks kinking, airway trauma, and aspiration of tape fragments. The
cuff remains unprotected of course and should be filled with
methylene blue stained saline so that perforation may be quickly
recognised.
Special ETT's. Some special tubes have been made to deal
with the problems of flammability and cuff rupture. From the
literature it doesn't appear that these are much better than a taped
tube but I'll describe them anyway.
- Norton. This spiral wound stainless steel ETT had no
cuff but a separate cuff could be attached if desired. It is no
longer available.
- Bivona Fome-Cuff. This is an aluminium spiral tube with
a silicone polyurethane foam cuff in a silicone envelope. The foam
is self inflating (it has to be sucked down) thus preventing
deflation in the event of cuff rupture. It should nonetheless be
filled with coloured saline to identify rupture. Its problem is
the trauma an undeflated cuff will cause in the event of
perforation. It also has a high incidence of sore throat and is
only recommended for use with a CO2 pulsed laser.
- Xomed Laser-Shield. A silicone elastomer tube
containing metallic powder only for use with pulsed CO2
laser less than 25W. There is still a risk of perforation and
fragmentation into silica ash and wet pledgets should be placed
around the cuff.
- Mallinckrodt Laser-Flex. An airtight stainless steel
spiral wound tube with two PVC cuffs which should be filled with
coloured saline. The distal cuff maintains the seal if the
proximal one is ruptured. It is only recommended for
CO2 and KTP-Nd-YAG, not the ordinary YAG.
Airway Fire Protocol.
- Remove source of fire (the laser!).
- Stop ventilating, disconnect circuit, extubate.
- Extinguish fire in bucket of water (MUST have one
ready!).
- Mask ventilate with 100% O2, continue anaesthesia
i.v.
- Direct laryngoscopy & rigid bronchoscopy for damage and
debris.
- Reintubate if damage.
- Blowtorch fire may need distal fibreoptic bronchoscopy and
lavage.
- Severe damage may need low tracheostomy.
- Assess oropharynx and face.
- CXR.
- ?Steroids.
Techniques Without ETT's. Spontaneous ventilation via
ventilating bronchoscopes using 100% O2, halothane and
topical anaesthesia (most important in paediatrics) is one
alternative but the vocal cords are not immobilised and there are
problems with air dilution and scavenging. Venturi jet ventilation
via bronchoscope, Carden tube or Benjet tube is another option. Its
advantages are the good conditions for laryngeal microsurgery and
reduced fire risk. It does however require i.v. maintenance and
muscle relaxation and potential problems are barotrauma, stomach
inflation, unprotected airway, respiratory obstruction and mucosal
dehydration.
HAPPY ZAPPING!