Chris Thompson USyd Lectures Listing Anaesthesia Breathing Systems
1. FUNCTIONS
2. CLASSIFICATION
Alternative - Conway
3. MAPLESON CIRCUITS
1. MAPLESON A - (Magill) CIRCUIT FGF enters at the end remote from the patient, and there is a Heidbrink one-way pop-off valve at the mask end. Originally C-type systems were common; Magill designed the A circuit to get the bag away from the patient during faciomaxillary surgery.
(a) Spontaneous ventilation The patient inspires whatever is in the tube, using the bag as a volume reservoir. On expiration, the bag refills from a combination of expired gas going back up the corrugated tube and incoming fresh gas. When the bag is full, exhaled alveolar gas is vented from the exhale valve, and then during any expiratory pause, FGF pushes the remaining alveolar gas out. Theoretically FGF = 0.7 x Valv should prevent significant rebreathing because deadspace gas (fresh) is not wasted, but FGF = VA more reliably prevents rebreathing. Tube volume must exceed (Vt-Vd) or alveolar gas could contaminate the bag. Inadequate FGF causes rebreathing . Difficult to detect from the CO2 waveform alone - all that happens is that the rapid fall on inspiration is delayed. If VA exceeds tubing volume, CO2 enters the bag and will be seen on inspiration on the capnogram. (b) Controlled ventilation If the anaesthetist fully closed the valve while squeezing the bag and didn't open it until just before the bag filled, this circuit would be OK. More commonly the valve is partially closed - enough to permit adequate tidal volumes despite parallel loss of gas out the valve. FGF must be increased to compensate for gas lost during inspiration - typically 2.5x minute ventilation. c) the Lack system A co-axial Magill, with the expiratory valve brought coaxially back to the Fresh Gas outlet. Not popular due to inefficiency during controlled ventilation.
Inefficient. Once the bag is full during expiration, fresh gas is vented. Not suited for spontaneous breathing - rebreathing is inevitable (with CO2 entering the tubing or bag) unless FGF exceeds peak inspiratory flow rates (3xMV). The C circuit is compact and was used for short transports before self-inflating bags became available. Acceptable CO2 levels could be achieved with a FGF of 2 x MV and mild hyperventilation. If the cylinder became empty ventilation was impossible.
3. MAPLESON D, E and F SYSTEMS FGF enters at patient end. D system has a relief valve proximal to the bag. Bain circuit is a co-axial D introduced in 1972 (Bain and Spoerel). E and F are functionally identical. Spontaneous breathing: inefficient. Inspiration is from Fresh Gas Flow and/or tube contents. If FGF > PIFR, all inspired gas will be fresh. If there is an expiratory pause, fresh gas pushes exhaled alveolar gas down the tube during the zero flow period, and FGF requirements are reduced somewhat. If no exp.. pause, needs FGF > 2.5xMV. With exp. pause may be OK as low as 100ml/kg. Most patients can readily manage a small inspired CO2 load. CO2 during capnometry inspiration indicates a need for higher flows. Controlled ventilation: more efficient. Significant mixing occurs and CO2 is 'washed out' by FGF. Provided that VA is adequate or slightly increased, CO2 washout depends on FGF, with normal CO2's at an FGF of 70ml/kg. Tubing + bag volume must exceed Vt to prevent air entrainment (unless functionally extended by a scavenging hose). Jackson-Rees modification of Ayre's T-Piece (Mapleson F) Original T-piece by Phillip Ayre in 1937 for children; ventilation by occlusion of the open ended tube with fresh gas entering at a right angle to the tube.. Modified by Jackson Rees in 1950's by adding an open-ended 500 ml bag to allow respiratory monitoring and/or assistance, and a parallel entry of the fresh gas line at the patient connection. Commonly used for paediatrics, esp.. neonates:
Deadspace is determined by the distance between fresh gas inflow point and the face. Specialised neonatal T-pieces direct FGF directly at the lips.. Disadvantages
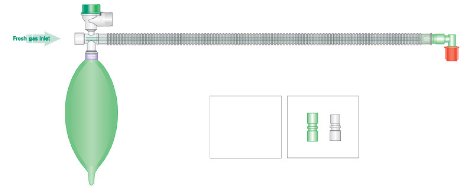
Bain Circuit Outer tube 22 mm diameter. 1.8m long. FGF travels to patient end via thinner 'coaxial' inside the expiratory tube. Advantages :
Disadvantages
4. CO2 ABSORPTION (CIRCLE) CIRCUITS Semi-closed and closed operation possible. 1. Absorber and absorbent Canister containing absorbent may be single or dual, of metal, glass or plastic. Air space typically 50% of total. Larger cross-sectional diameters allow less turbulence with reduced resistance and less dust. Well packed canisters allow diffuse spread of gas through the absorbent, rather than in a columnar fashion. Bypass mechanism can isolate absorber from circuit and allow PaCO2 to rise without decreasing minute ventilation. Advantages of CO2 absorption
Soda lime
Heat in the canister is heat of neutralisation; liberates water vapour; may indicate high patient VCO2 e.g. MH Signs of exhaustion
2. Fresh gas inlet Usually between CO2 absorber and inspiratory valve. 3. Uni-directional valves
4. APL (adjustable pressure limit) valve
5. Pressure gauge/s
6. Breathing hoses
7. Reservoir bag
8. "Y" Piece Standard 22 mm male connections for breathing hoses. Patient connection port is a 15 mm female fitting or a 15 mm female port coaxial within a 22 mm male fitting. Common source of leaks. 9. O2 Analyser
10 Ports
See Also: Equipment notes by Mark Finnis |
||||||||

 2. MAPLESON B & C SYSTEMS
2. MAPLESON B & C SYSTEMS